

4. The District Management Team
5.58 The Canterbury and Thanet Health District covers an area of 288 square miles and includes 21 hospitals containing 3,500 beds which were previously managed by three Hospital Management Committees and two local authorities. After considerable argument it was finally decided that the team should include an elected Consultant and General Practitioner from both Thanet and Canterbury District Medical Committees. When the Community Physician is added this results in a District Management Team comprising the Administrator, the Finance Officer, the Nursing Officer and five doctors. No member of the Team has any psychiatric experience and the doctors have insufficient time to familiarise themselves with the hospitals they try to manage. The Consultant member of the Team who gave evidence to us had attended meetings at St. Augustine's but had not had time to visit any part of it.
5.59 The District Management Team's task is enormous, and it is totally unrealistic to imagine that it will ever be able to fill the gap left by the Management Committees. Indeed, everyone seemed to be agreed that it could only function if most of the management is carried out by the hospitals under authority delegated by the Team.
5.60 We set out below some of the ways in which the District Management Team failed to get to grips with the problems of St. Augustine's, and then try to identify some of the causes for this failure in addition to the obvious one of shortage of time.
(a) Empty beds
5.61 On October 31st, 1975, after allowing for patients on leave, there were 160 empty beds in the hospital. This was not unusually high and the numbers had been running at about 130 for a considerable time. The District Management Team was unaware of this although it had authorised considerable expenditure for upgrading the Elder complex to provide more beds. It had not apparently contemplated reorganising the allocation of beds to reduce the overcrowding and pressure on the staff in some wards. Nor had it collected any statistics to enable it to assess bed usage on admission wards, beds available throughout the hospital and other relevant factors.
(b) Uneven work load for Areas (Divisions)
5.62 It is impossible to walk round St. Augustine's using one's eyes and talking to the staff without becoming rapidly aware that Clinical Area 1 seems, and is considered, to be much better off in all respects than the other two areas, particularly Clinical Area 2 which is regarded as the Cinderella. A careful check should have been kept to see whether any adjustments were needed to the geographical areas or the resources allocated to them. The following table provides statistics which demand careful consideration by the hospital and the District Management Team:
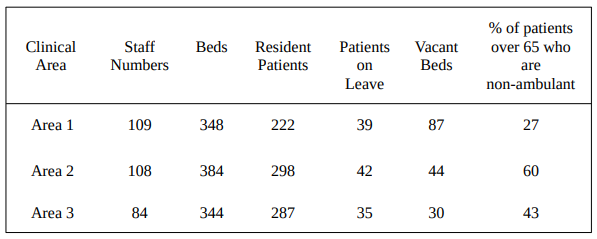
5.63 It may be that examination of the problem will reveal that no adjustments are needed. The point we make is that the District Management Team were not aware that there was anything requiring examination.
(c) Shortage of Occupational Therapy
5.64 This is a problem which was known to the District Management Team, and at the request of the Head Occupational Therapist it authorised the employment of four additional untrained Aides. This, however, was not really dealing with the problem. It should have appreciated that there is no reasonable prospect of recruiting the qualified staff required and asked the hospital to produce alternative plans, based upon a realistic assessment of the numbers and categories of staff which it could reasonably expect to recruit.
(d) The Critique
5.65 It failed to ask the right questions and too easily accepted the answers of those criticised. (See paragraphs 4.81-2, 4.91-8, 4.110,111).
(e) The balance between the medical and other professions
5.66 In asking the Chairman of the Medical Executive Committee, but not the Divisional Nursing Officer, to attend its meetings it has overemphasized the role of the Doctors. Indeed it has sought to use the Medical Executive Committee as the management team for the hospital without sufficiently appreciating that that Committee's concern is with medical matters and that it feels unable, for reasons already set out, to do much managing. On the question of the continued use of the operating theatre, the District Management Team sought advice from doctors, but not, so far as we are aware, from the nurses in the hospital.
5.67 The District Administrator has been diligent in his visiting: for example he paid the hospital 69 visits between April and December, 1974; but on the whole he has not had the time or the knowledge to identify problems which are not presented to him, and his efforts to solve individual problems have sometimes obscured the wider picture.
5.68 A further factor limiting the District Management Teams effectiveness has been that it has not regarded itself as having any role, on the clinical side, even in policy making. We asked the District Administrator "Where do you draw the line on a long stay ward, which is what the Critique has been concerned with, between a clinical matter and a non, clinical matter?" He replied "It is very difficult to do so. You can only go on the view of your medical colleagues." We asked a Consultant member of the Team where he would draw the line in a long stay ward in St. Augustine's. He replied "That is a very difficult question for a radiologist to answer." We pressed him further, pointing out that on the answer might depend the power of the District Management Team to act, and he then said "With a long stay patient I presume that the Consultant would be responsible for the patient's general well being and that he would be responsible for matters that would impinge on the patient's continuing treatment." If, in fact, a District Management Committee is unable, as this one believes, to act in matters within the clinical autonomy of the Consultant, the wide limits placed by this Consultant on its boundaries would mean that the team was largely powerless in the long stay wards. If members of the District Management Team held differing views as to the limits of clinical autonomy, consensus decision taking would require that the matter be referred to the Area Team of Officers and the Area Health Authority for decision. While this procedure was being followed urgent matters within the Hospital requiring decision and action would have to wait. Such a system is certainly not conducive to effective management.
06 April 2026
![]()